Vernal keratoconjunctivitis (VKC)
Authors

The patient is a 6-year-old boy with seasonal conjunctival symptoms (exacerbation in the spring), associated to atopic eczema.
Previous treatment included topical eye drops (antihistamines, antibiotics & NSAIDs) with recurrence of the symptoms when the therapy is discontinued.
The atopic dermatitis is treated sometimes with deflazacort (Rosilan) and tacrolimus (Protopic).
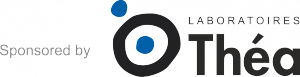
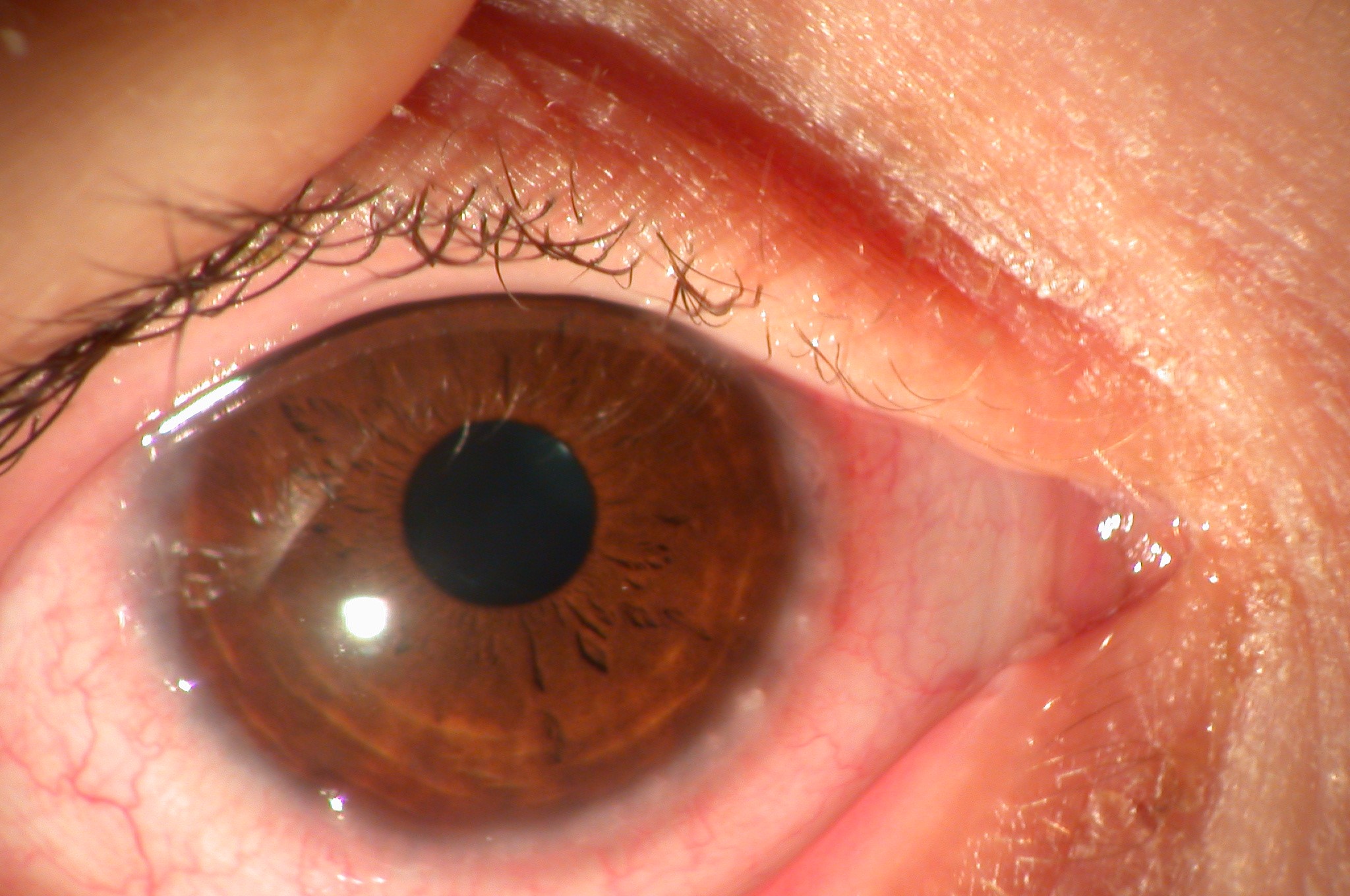
This patient presented marked photophobia, severe itching, tearing, foreign body sensation, mucous discharge, burning, with normal visual acuity.
Ptosis caused by drooping of the eyelids was present.
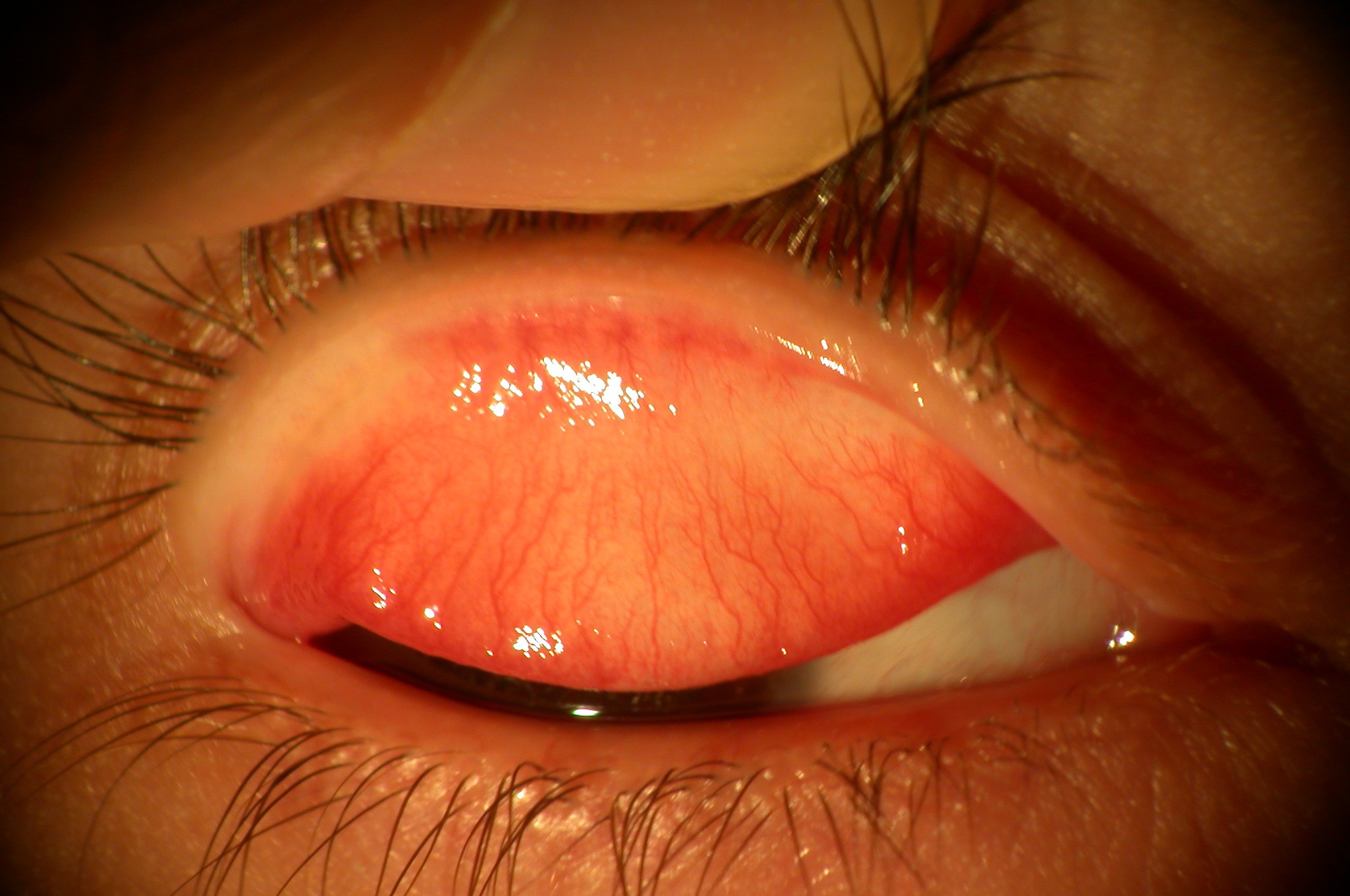
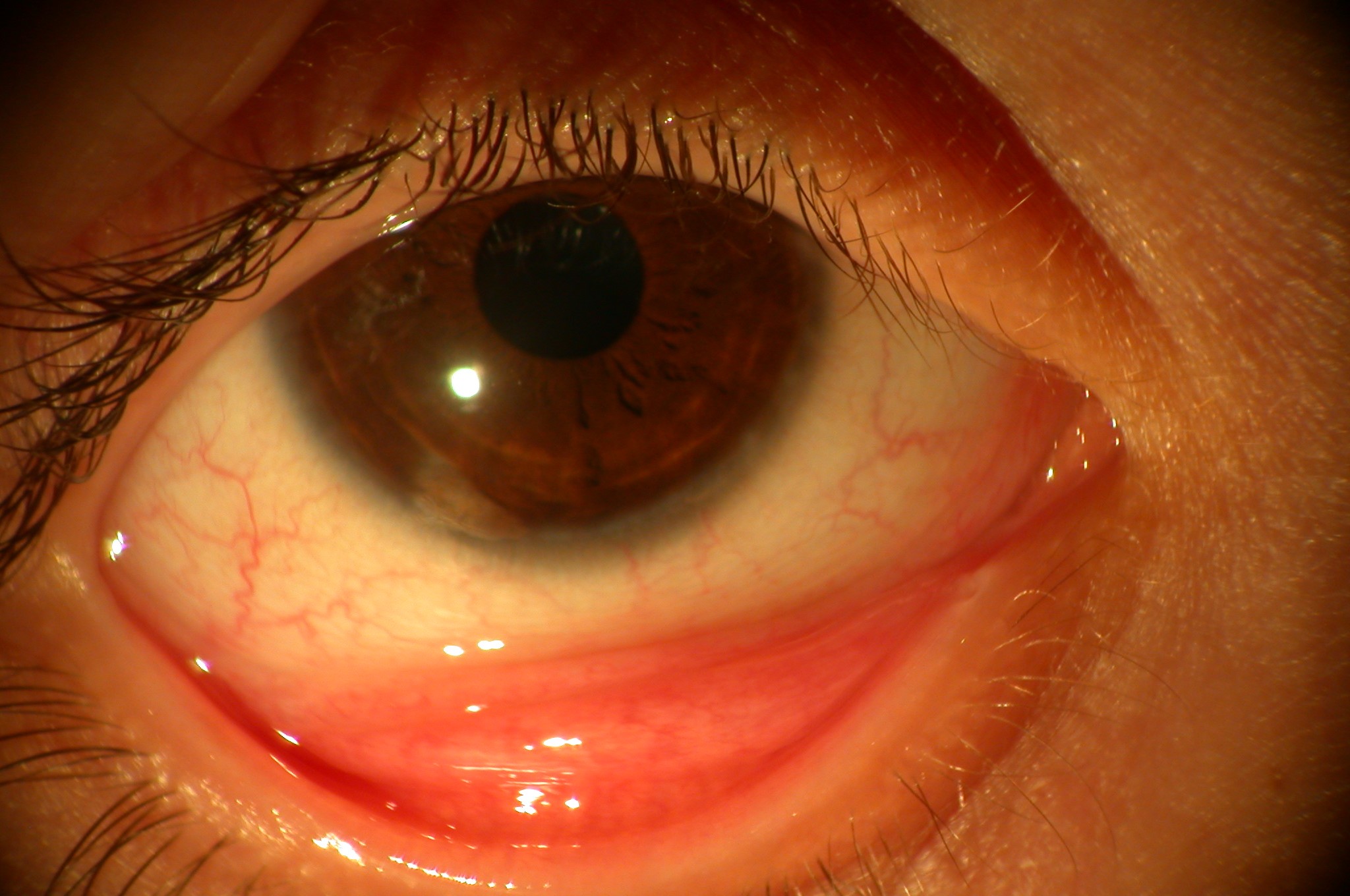
In Spring the eyelids showed mild oedema and blepharitis, the bulbar and tarsal conjunctiva was hyperaemic with papillary reaction, but without the typical giant cobblestone-like papillae.
The cornea showed mild punctate keratopathy and the limbal conjunctiva was thickened and oedematous, with limbal nodules with gelatinous appearance was observed – Trantas’ dots.
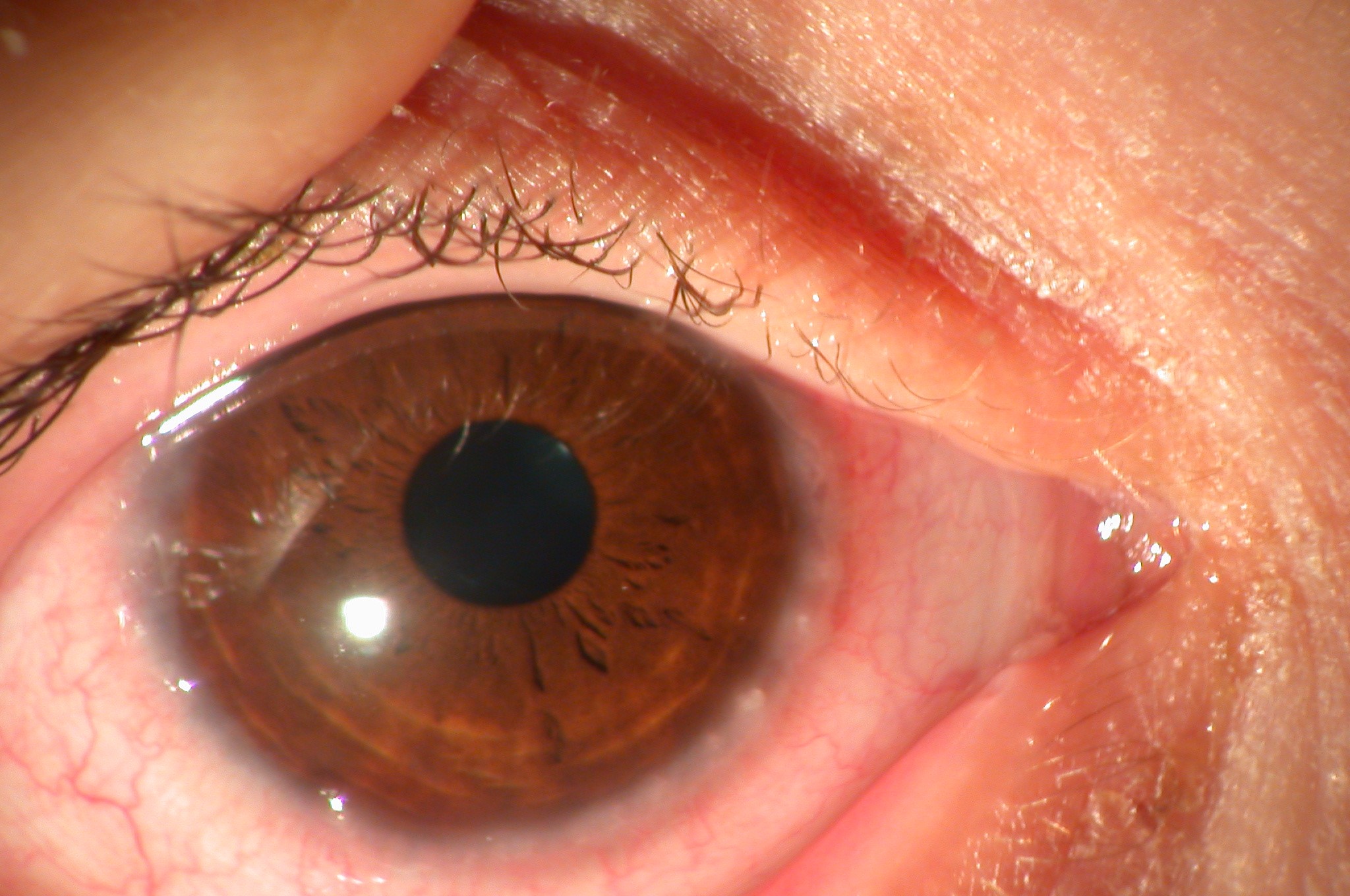
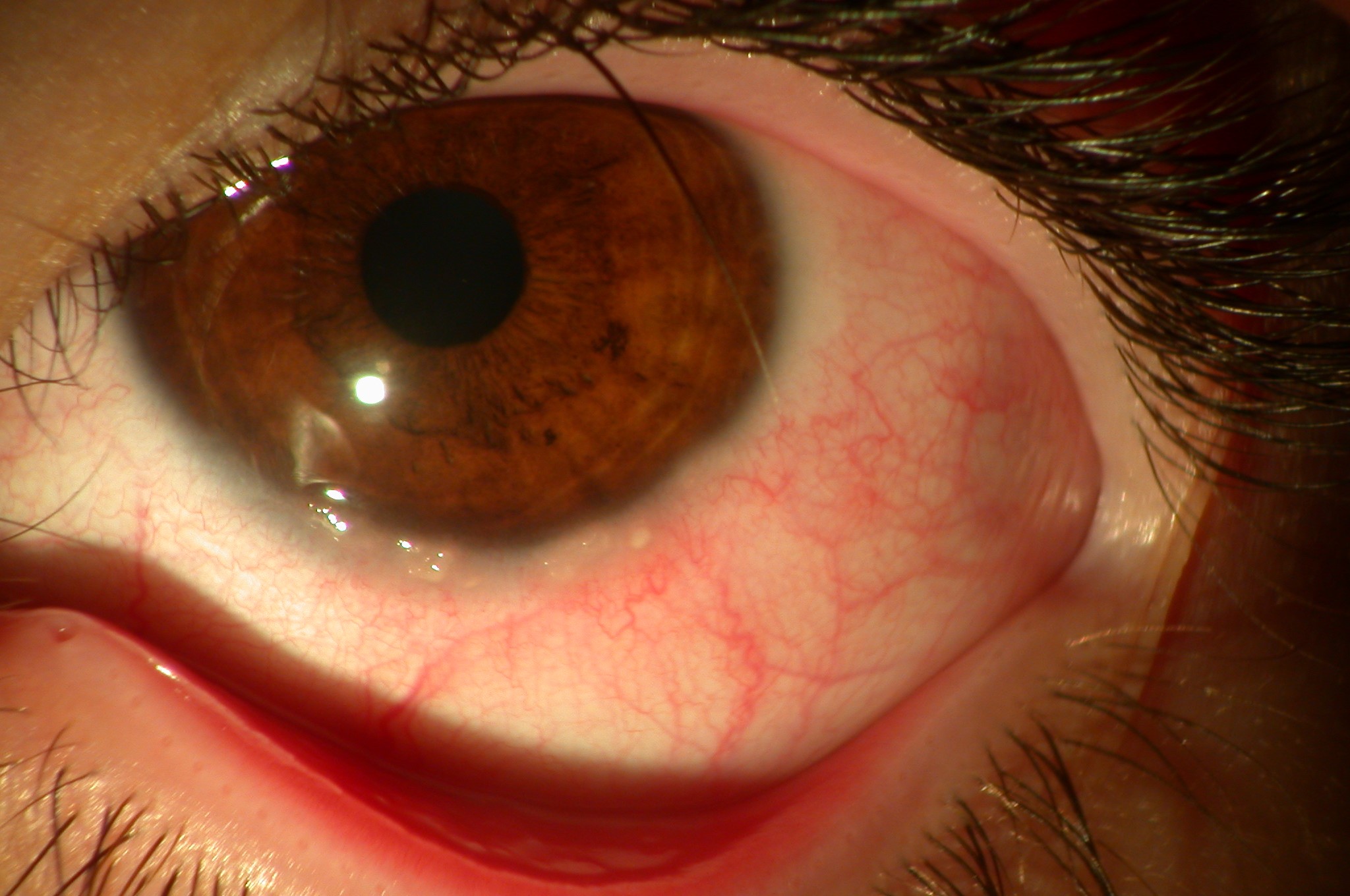
This young boy with allergic keratoconjunctivitis and Trantas’ dots at the limbus must have vernal limbal keratoconjunctivitis (VKC).
Conservative treatment with frequent use of cold compresses and proper eyelid hygiene was helpful.
A brief course of topical dexametasone (Dexafree) was used in the form of “pulse therapy” to control the flare-up of the disease.
Topical corticosteroids are the mainstay of therapy, but should be used with great caution, and must be limited for short periods, and monitored by ophthalmologists, because they are associated with corneal epithelium healing delay, development of cataracts, steroid-induced glaucoma and local immunosuppression with consequent superinfection, namely herpes.
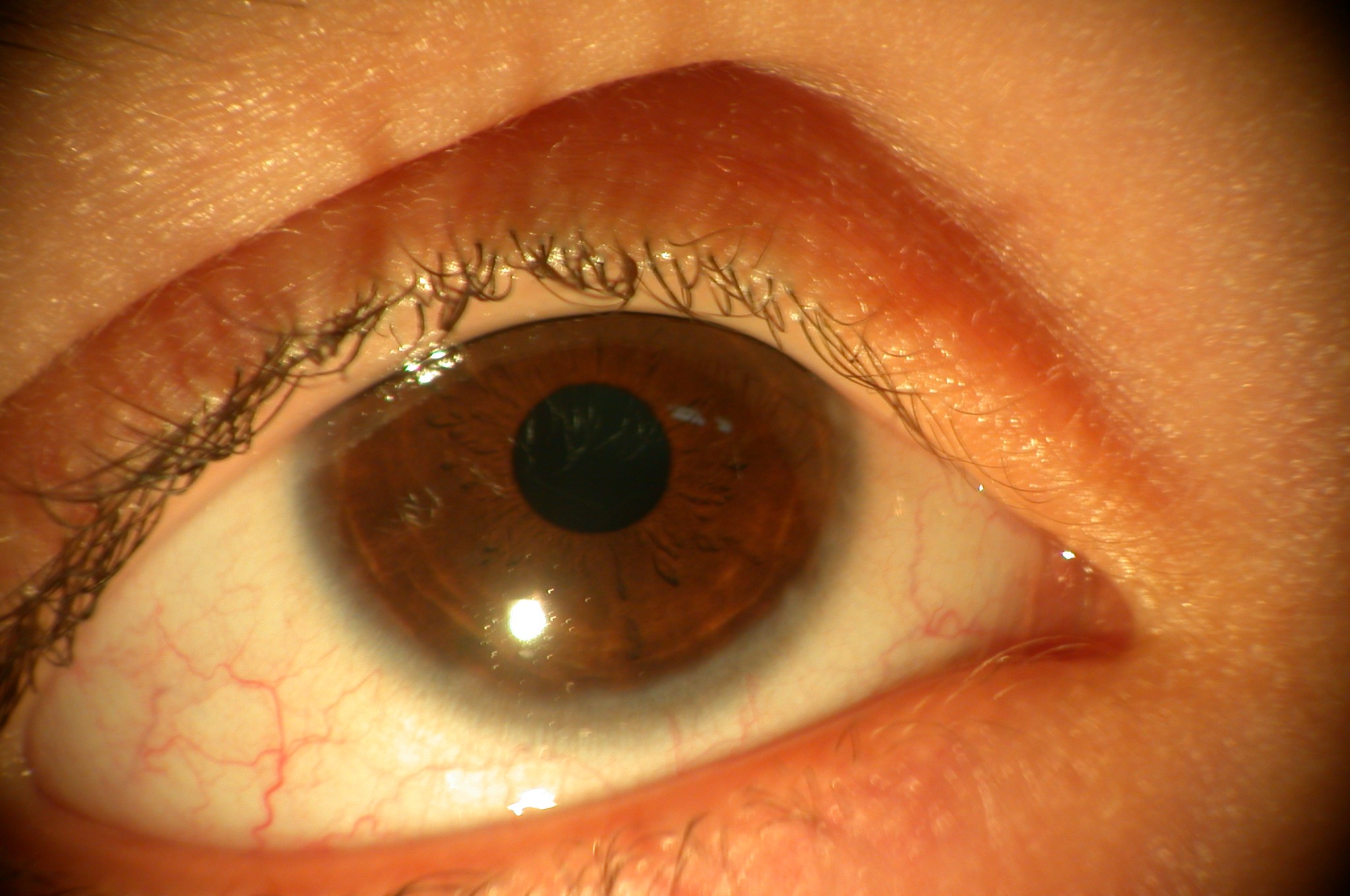
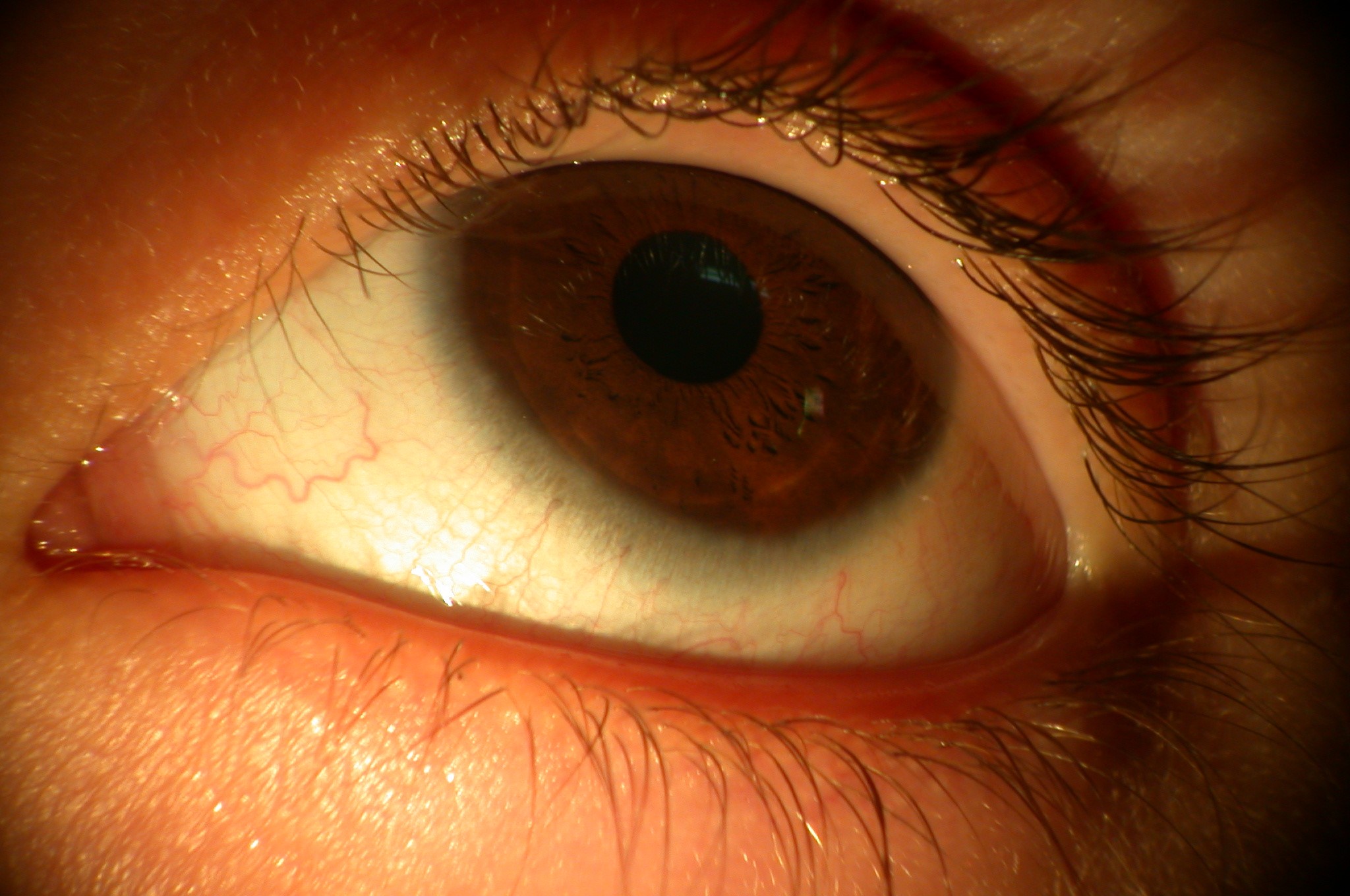
Three weeks after the first visit the photophobia and the conjunctival hyperaemia had decreased, and the limbal nodules disappeared.
Therapy for VKC should be aimed primarily at the identification of the allergen and, when possible, its elimination or avoidance. While these patients generally have multiple sensitivities to such allergen as grasses, dust, and mites, avoidance of certain environments, such as warm, Mediterranean areas, can be helpful in acute exacerbations. Avoidance of wind, which is usually pollen bearing, and the use of glasses or goggles to decrease airborne allergen contact.
Because VKC eventually resolves without scarring, treatment should be conservative in order to avoid serious iatrogenic side effects and topical mast-cell stabilizers are an important adjunct to the pharmacologic arsenal for allergic conjunctivitis.
In giant papillae of VKC, the extracellular matrix is characterized by overproduction of collagens. Expression of growth factors in the conjunctiva by resident cells (mast cells, epithelial and endothelial cells) and inflammatory cells (macrophages, eosinophils) may contribute to papillae formation and fibrosis evolution in chronic allergic diseases.
Generally, VKC is self-limited, chronic, and sometimes severe; however, it usually resolves around puberty without treatment.
VKC is an ocular allergic disease of the conjunctiva with affects particularly boys under 14 years of age. If corneal involvement is present and persists in the visual axis, it can result in permanent visual damage.
Ophthalmologists and allergologists must work in concert to address the underlying allergic disorder and prevent loss of vision.
Aggressive treatment early in the course of the disease is preferable, because the disease is harder to control after a chronic course.